Prescription drug pricing in the United States has long been a focal point of health policy debate. For Medicare beneficiaries, particularly older adults and individuals living with chronic conditions, out-of-pocket drug costs can pose significant financial strain. At the same time, Medicare spending on prescription drugs has continued to rise, driven by increased utilization of high-cost specialty therapies and elevated launch prices for innovative treatments. These trends have raised concerns not only about patient affordability, but also about the long-term fiscal sustainability of the Medicare program.
The Inflation Reduction Act (IRA) introduced one of the most significant changes to Medicare drug pricing policy in decades by granting Medicare limited authority to directly negotiate prices with manufacturers for a select group of drugs. Since enactment, "Medicare drug price negotiation" has become a prominent topic across policy, industry, and investment discussions. However, the scope and mechanics of the program are often misunderstood.
This brief guide outlines the practical mechanics and limitations of Medicare drug price negotiation under the IRA. Readers seeking a more detailed analysis of implementation cycles, policy nuances, and system‑level implications across the healthcare ecosystem can explore these topics further in our full white paper below.
Medicare Drug Pricing Before the IRA
To understand the significance of the IRA, it is important to first understand how Medicare drug pricing functioned historically.
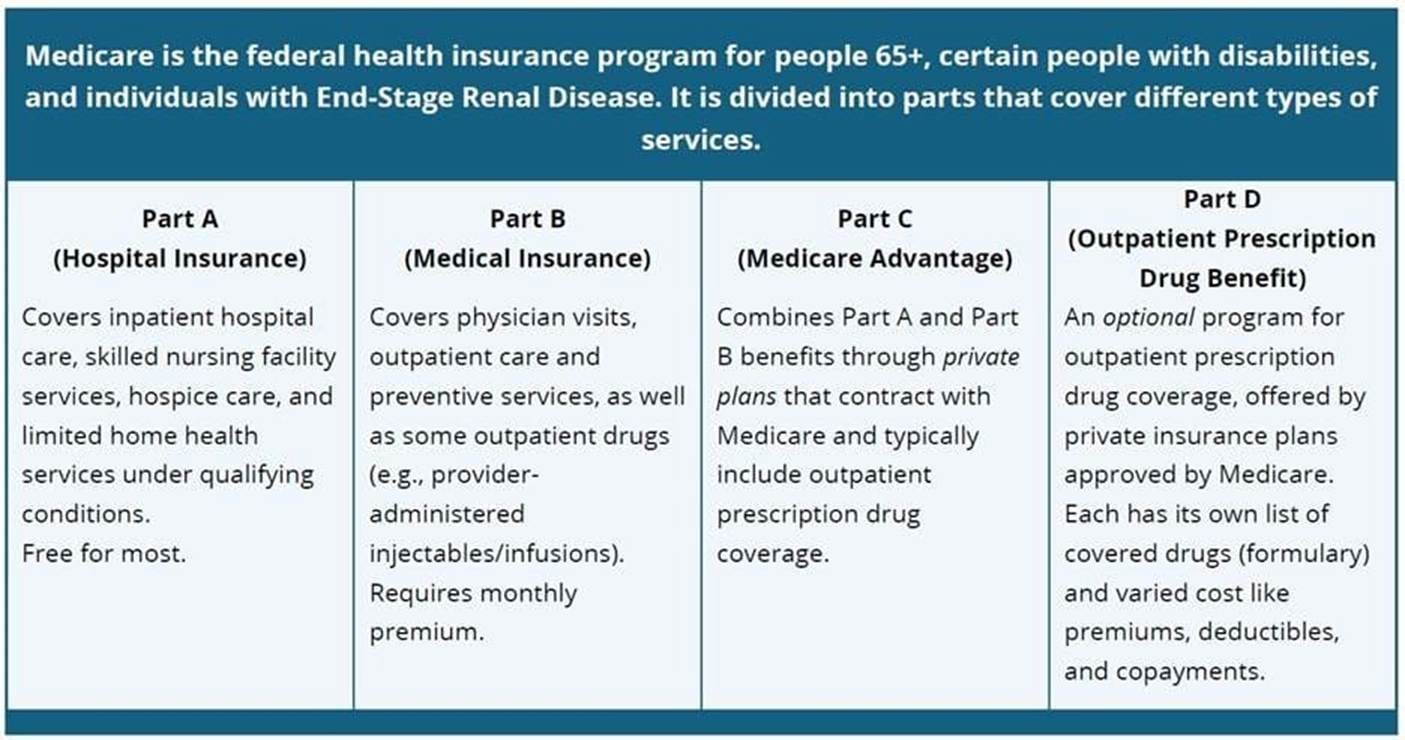
Medicare Part D, which covers outpatient prescription drugs, was intentionally designed as a market‑based program. Private Part D plans develop formularies and negotiate price concessions with manufacturers, frequently through pharmacy benefit managers (PBMs). Federal law included a statutory “non‑interference clause” that prohibited the Department of Health and Human Services (HHS) from directly intervening in these negotiations.
The underlying rationale was that competition among private plans would help manage costs while preserving beneficiary access and incentives for pharmaceutical innovation. However, over time, structural limitations became increasingly evident. Prior to the IRA, Part D lacked a hard annual cap on beneficiary out‑of‑pocket spending, leaving patients using high‑cost therapies exposed to substantial financial risk.
What Changed Under the IRA?
The IRA established a Medicare Drug Price Negotiation Program, administered by HHS through the Centers for Medicare & Medicaid Services (CMS). Under this program, CMS may negotiate prices directly with manufacturers for a limited number of high‑expenditure drugs.
Importantly, the IRA does not create universal price negotiation across all Medicare‑covered drugs. The vast majority of products continue to operate under the existing market‑based framework. Instead, the program is narrowly targeted to drugs that:
- Account for significant Medicare spending, and
- Lack generic or biosimilar competition
This targeted design reflects a policy compromise—seeking to moderate spending growth where competition is unlikely to emerge in the near term, while minimizing disruption in other segments of the market.
How Are Drugs Selected for Negotiation?
CMS follows a structured, multi‑step selection process rather than simply targeting the most expensive drugs.
The process applies statutory eligibility criteria and exclusions to narrow the candidate pool. Drugs may be excluded if they:
- Are too new (within defined post‑approval timeframes)
- Face existing generic or biosimilar competition
- Meet other exclusion criteria specified in the statute
Only after these filters are applied does CMS identify the final set of drugs subject to negotiation. This approach is designed to focus negotiation on products that drive Medicare spending while avoiding premature intervention in competitive or emerging markets.
What Happens During the Negotiation Process?
Once CMS publishes a selected‑drug list, manufacturers enter a formal negotiation process that includes structured evidence submission and iterative price discussions.
Manufacturers are required to submit information related to:
- Research and development investments
- Production and distribution costs
- Sales, revenue, and market data
- Patent and exclusivity status
CMS may also consider broader contextual factors, including therapeutic alternatives, clinical benefit, unmet medical need, and impacts on specific patient populations. The outcome of this process is a negotiated price that applies within Medicare.
Implementation Status and Timeline
The Medicare Drug Price Negotiation Program has been implemented through phased negotiation cycles, rather than as a single, system‑wide change.
The initial cycle focused on ten high‑expenditure Part D drugs used to treat prevalent conditions such as diabetes, cardiovascular disease, autoimmune disorders, and cancer. Subsequent cycles have expanded the program to include additional therapies, including high‑cost GLP‑1 medications and oncology drugs. Future phases will begin incorporating Medicare Part B drugs, such as provider‑administered therapies commonly used in oncology and immunology.
This gradual rollout allows CMS, manufacturers, and other stakeholders to adapt to the new framework over time.
Why This Matters
Although the Medicare Drug Price Negotiation Program applies to a limited number of drugs, its implications extend well beyond the selected products and have meaningful consequences for manufacturers, investors, and the broader healthcare ecosystem.
- For patients, the most immediate impact is expected to be improved affordability through lower negotiated prices and reduced out‑of‑pocket spending for selected high‑expenditure therapies.
- For manufacturers, the program introduces durable changes to long‑term product strategy. Negotiation risk is now a predictable lifecycle milestone for certain products, influencing decisions around launch pricing, indication sequencing, evidence generation, and timing of generic or biosimilar entry. The policy increases the strategic value of robust comparative effectiveness, real‑world evidence, and differentiated clinical benefit—particularly for products with prolonged market exclusivity.
- For investors and the healthcare system, the IRA represents a structural shift in federal involvement in drug price formation. While preserving Medicare’s largely market‑based foundation, the negotiation framework introduces new policy‑driven constraints that affect asset valuation, revenue durability, and portfolio risk—particularly for late‑lifecycle, high‑expenditure products without near‑term competition.
The Bottom Line
The Medicare Drug Price Negotiation Program does not represent a wholesale redesign of pharmaceutical pricing in the United States. Instead, it establishes a targeted, evidence‑driven mechanism to address spending growth in areas of concentrated Medicare expenditure, while attempting to balance affordability, sustainability, and innovation.
For a deeper discussion of implementation mechanics, policy nuances, and downstream implications for manufacturers and healthcare stakeholders, download the full white paper below.
Other Posts You Might Like